
Case 1
Clinical Stem:
You are a third-year medical student on a rural hospitalist rotation in Lloydminster. A 56-year-old male presents to the emergency department with a 3 day history of non-productive cough and fevers. He reports feeling increasingly fatigued and has had some mild pleuritic chest discomfort localized to the right side. He denies hemoptysis, recent travel, or sick contacts. He is a lifelong non-smoker and has no significant past medical history.
On examination, he appears mildly unwell. His vital signs are as follows:
-
Temperature: 38.3°C
-
Heart Rate: 94 bpm
-
Respiratory Rate: 20 breaths/min
-
Blood Pressure: 128/76 mmHg
-
SpO₂: 94% on room air
On auscultation, breath sounds are decreased over the right mid-lung zone anteriorly, with bronchial breath sounds and dullness to percussion in the same area. No wheezes or crackles are noted elsewhere.
Your preceptor asks you to order a posterior-anterior and lateral chest X-ray for further evaluation.
Question:
Review the provided chest radiograph (PA and lateral views). What abnormalities do you observe, and what is your most likely diagnosis based on these imaging findings?
PA View
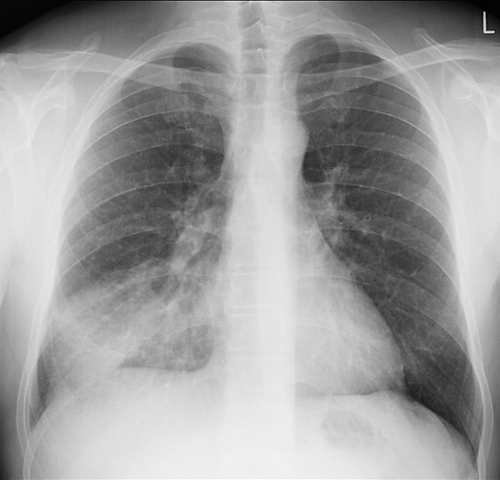
Sorrentino, S. A. (n.d.). Radiopaedia case rID: 14979. Radiopaedia.org. https://radiopaedia.org/cases/14979?lang=us[AS1]
Lateral View

Sorrentino, S. A. (n.d.). Radiopaedia case rID: 14979. Radiopaedia.org. https://radiopaedia.org/cases/14979?lang=us[AS1]
Chest X-Ray Interpretation Using RIPE + ABCDE
Step 1: R.I.P.E. – Technical Adequacy
-
Rotation
-
Clavicles are equidistant from the spinous processes.
-
Not rotated → accurate anatomical relationships.
-
-
Inspiration
-
9-10 posterior ribs visible above the diaphragm.
-
Good inspiratory effort.
-
-
Projection
-
Posterior-Anterior (PA) view.
-
Heart size is reliable here.
-
-
Exposure
-
Vertebral bodies visible behind the heart shadow.
-
Adequately penetrated.
-
Step 2: A – Airway & Mediastinum
-
Trachea is midline, no deviation.
-
Carina visible, no airway obstruction.
-
Silhouette Sign:
-
Right heart border is silhouetted, suggesting loss of interface between the right heart and adjacent lung → indicative of right middle lobe pathology.
-
Step 3: B – Breathing (Lungs & Pleura)
-
Increased opacity in the right mid-zone (PA view).
-
Lateral view shows a triangular/wedge-shaped opacity between the horizontal and oblique fissures—classic for right middle lobe involvement.
-
No cavitation, no pleural effusion, and no pneumothorax.
-
Lung markings preserved elsewhere.
Step 4: C – Circulation (Heart & Vessels)
-
Heart size normal (cardiothoracic ratio <50% on PA view).
-
Right heart border not visible → reinforces silhouette sign due to middle lobe consolidation.
-
Aortic knob and pulmonary vasculature appear normal.
Step 5: D – Diaphragm
-
Right hemidiaphragm higher than left (normal).
-
No free air under diaphragm.
-
Costophrenic angles sharp → no pleural effusion.
-
Gastric bubble visible under the left hemidiaphragm.
Step 6: E – Everything Else
-
Bones: No rib or clavicle fractures. Spine is intact.
-
Soft tissues: No subcutaneous emphysema or masses.
-
No lines, tubes, or devices seen in this image.
Summary
The CXR demonstrates a focal opacity in the right mid-lung zone, which silhouettes the right heart border on PA view and is localized to the space between the horizontal and oblique fissures on lateral view, consistent with right middle lobe consolidation.
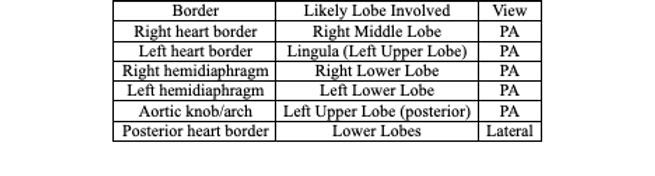
Key Teaching Points
Border | View | Likely Lobe Involved |
|---|---|---|
Posterior heart border | Lateral | Right Middle Lobe |
Aortic knob/arch | PA | Lingula (Left Upper Lobe) |
Left hemidiaphragm | PA | Right Lower Lobe |
Right hemidiaphragm | PA | Left Lower Lobe |
Left heart border | PA | Left Upper Lobe (posterior) |
Right heart border | PA | Lower Lobes |
•Always correlate imaging findings with the clinical scenario.
Always correlate imaging findings with the clinical scenario.